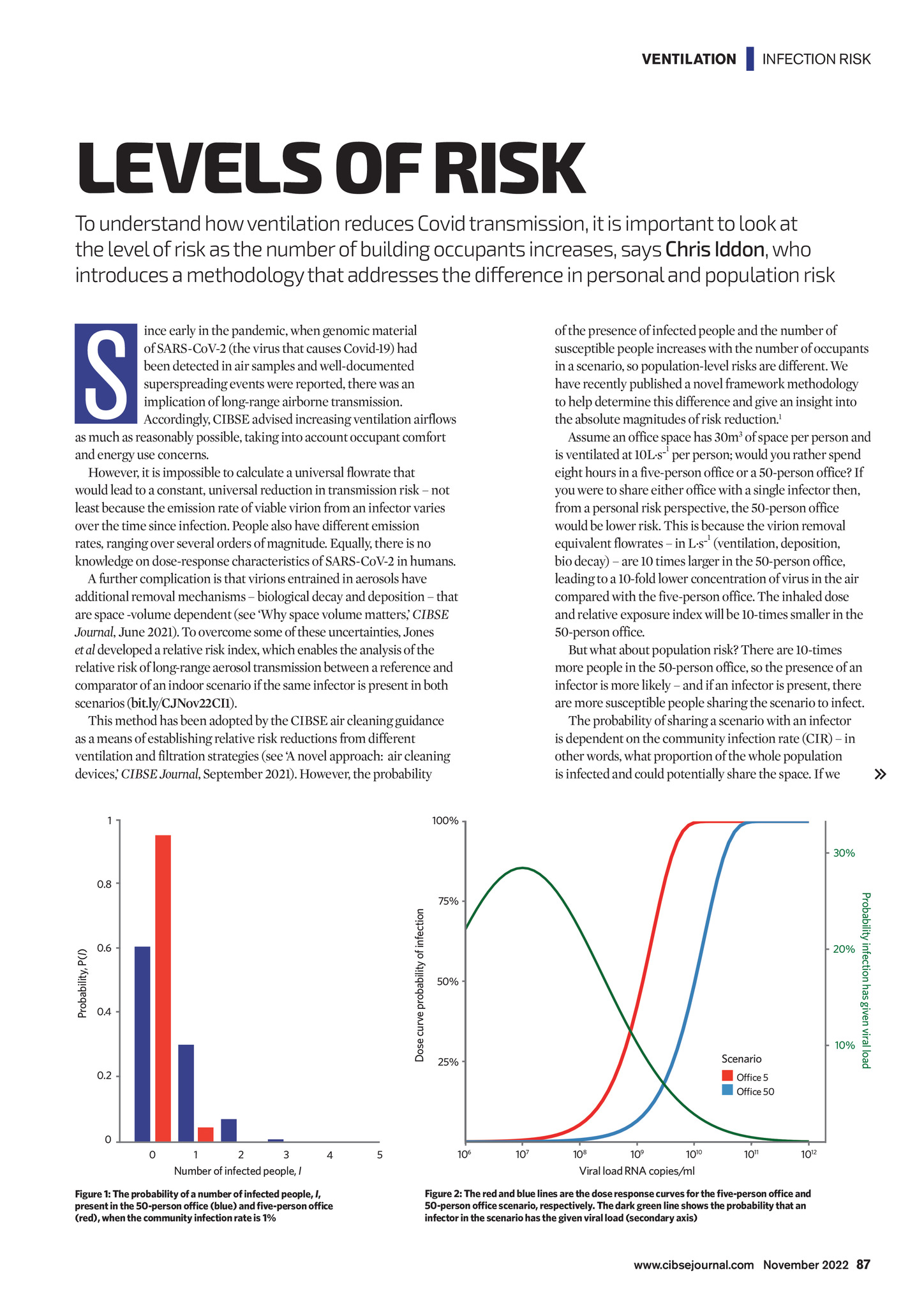
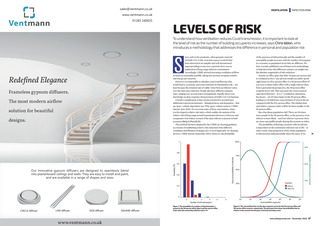
VENTILATION | INFECTION RISK LEVELS OF RISK To understand how ventilation reduces Covid transmission, it is important to look at the level of risk as the number of building occupants increases, says Chris Iddon, who introduces a methodology that addresses the difference in personal and population risk S ince early in the pandemic, when genomic material of SARS-CoV-2 (the virus that causes Covid-19) had been detected in air samples and well-documented superspreading events were reported, there was an implication of long-range airborne transmission. Accordingly, CIBSE advised increasing ventilation airflows as much as reasonably possible, taking into account occupant comfort and energy use concerns. However, it is impossible to calculate a universal flowrate that would lead to a constant, universal reduction in transmission risk not least because the emission rate of viable virion from an infector varies over the time since infection. People also have different emission rates, ranging over several orders of magnitude. Equally, there is no knowledge on dose-response characteristics of SARS-CoV-2 in humans. A further complication is that virions entrained in aerosols have additional removal mechanisms biological decay and deposition that are space -volume dependent (see Why space volume matters, CIBSE Journal, June 2021). To overcome some of these uncertainties, Jones et al developed a relative risk index, which enables the analysis of the relative risk of long-range aerosol transmission between a reference and comparator of an indoor scenario if the same infector is present in both scenarios (bit.ly/CJNov22CI1). This method has been adopted by the CIBSE air cleaning guidance as a means of establishing relative risk reductions from different ventilation and filtration strategies (see A novel approach: air cleaning devices, CIBSE Journal, September 2021). However, the probability 1 of the presence of infected people and the number of susceptible people increases with the number of occupants in a scenario, so population-level risks are different. We have recently published a novel framework methodology to help determine this difference and give an insight into the absolute magnitudes of risk reduction.1 Assume an office space has 30m3 of space per person and 1 is ventilated at 10L.s- per person; would you rather spend eight hours in a five-person office or a 50-person office? If you were to share either office with a single infector then, from a personal risk perspective, the 50-person office would be lower risk. This is because the virion removal 1 equivalent flowrates in L.s- (ventilation, deposition, bio decay) are 10 times larger in the 50-person office, leading to a 10-fold lower concentration of virus in the air compared with the five-person office. The inhaled dose and relative exposure index will be 10-times smaller in the 50-person office. But what about population risk? There are 10-times more people in the 50-person office, so the presence of an infector is more likely and if an infector is present, there are more susceptible people sharing the scenario to infect. The probability of sharing a scenario with an infector is dependent on the community infection rate (CIR) in other words, what proportion of the whole population is infected and could potentially share the space. If we 100% 30% Dose curve probability of infection 0.6 0.4 0.2 75% 20% 50% 10% Scenario 25% Office 5 Office 50 Probability infection has given viral load Probability, P(I) 0.8 0 0 1 2 3 4 Number of infected people, I Figure 1: The probability of a number of infected people, I, present in the 50-person office (blue) and five-person office (red), when the community infection rate is 1% 5 106 107 108 109 1010 1011 1012 Viral load RNA copies/ml Figure 2: The red and blue lines are the dose response curves for the five-person office and 50-person office scenario, respectively. The dark green line shows the probability that an infector in the scenario has the given viral load (secondary axis) www.cibsejournal.com November 2022 87 CIBSE Nov 22 pp87-88 Chris Iddon ventilation.indd 87 21/10/2022 19:15